
מאמרים על חלומות
DREAM THEORIES AND SCIENCE OF DREAMING / Dr. Raz Even
facebook Email : razeven.dreams-at-gmail.com

תורת החלומות בעריכת רז אבן
Creativity in Dreams – Problem-Solving and Innovation
In Chapter 7 of "Altered States of Dreaming: Structure and Logic," We expand on the…

תורת החלומות בעריכת רז אבן
שפת החלום במבט סטרוקטורליסטי: בין מיתוס, מבנה ומשמעות
שפת החלום במבט סטרוקטורליסטי: בין מיתוס, מבנה ומשמעות החלום, בדומה למיתוס, פועל על פי היגיון…
תורת החלומות בעריכת רז אבן
The Fabric of Dreams: Symbolism, Logic, and the Structural Unconscious
I. Introduction: Deciphering the Dreamscape - Symbolism and Logic in the Nocturnal Mind The landscape…
תורת החלומות בעריכת רז אבן
החלון כקרע אפיסטמולוגי
החלום כקרע אפיסטמולוגי -:אינטגרציה בין נוירופסיכואנליזה לתיאוריה ביקורתית החלום אינו רק ראי לנפש – הוא…
תורת החלומות בעריכת רז אבן
Brain networks and dreaming
⸻ V. Toward Network-Based Models: Contemporary Alternatives to the Lateralization Framework While the study of…
תורת החלומות בעריכת רז אבן
Dreaming and the Spectrum of Consciousness
I. Introduction The website DreamTheory.org, edited by Dr. Raz Even, serves as a comprehensive digital…
תורת החלומות בעריכת רז אבן
Key Themes and Insights from DreamTheory.org:
Lucid Dreaming and Psychoanalysis: Lucid dreams provide a unique context for psychoanalytic exploration, allowing for…

תורת החלומות בעריכת רז אבן
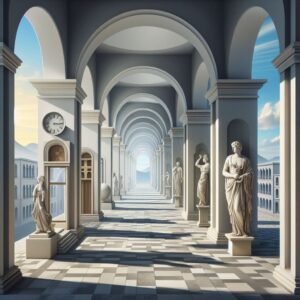
Giorgio de Chirico’s art – PSYCHOANALYSIS and DREAM SPACE
Giorgio de Chirico's art is a profound narrative that leverages the uncanny and the architectural…
תורת החלומות בעריכת רז אבן
The website DreamTheory.org offers a rich exploration into various aspects of dream science
The website DreamTheory.org offers a rich exploration into various aspects of dream science and psychoanalysis,…
Consciousness
Dream science
Dreams
Lucid dreams
Neuropsychoanalysis
Neuropsychology
תורת החלומות בעריכת רז אבן
Freudian Theory and Modern Neuroscience
Integration of Freudian Theory and Modern Neuroscience Freud's psychoanalytic theory posits that dreams reveal latent…